Applying the ACLS Algorithm Under High-Stress Conditions

Advanced Cardiovascular Life Support (ACLS) training prepares clinicians to manage cardiac arrest and life-threatening arrhythmias through structured, evidence-based algorithms established by the American Heart Association. These algorithms organise rhythm recognition, defibrillation sequencing, medication timing, and mandatory reassessment into defined clinical pathways designed to preserve treatment accuracy during physiologically unstable events.
Cardiac arrest management demands simultaneous technical execution and coordinated oversight. Rhythm analysis must occur while compressions are maintained, medications are prepared, airway status is monitored, and haemodynamic response is interpreted in real time. Under these conditions, performance strain arises from cognitive load rather than lack of knowledge. Sequencing errors, delayed escalation, and inconsistent reassessment are common consequences when environmental intensity compresses decision-making capacity.
ACLS training addresses this performance vulnerability by embedding structured progression into arrest management. Instead of reconstructing treatment order from memory, clinicians operate within predefined checkpoints that regulate timing, escalation thresholds, and rhythm-specific intervention pathways.
ACLS Algorithm Structure as Decision Regulation
ACLS algorithms categorise resuscitation according to rhythm and haemodynamic stability. Each pathway defines when electrical therapy is indicated, when pharmacologic support is required, and when reassessment must occur. This organisation reduces ambiguity at the moment when ambiguity carries the greatest risk.
Precision in timing is not administrative; it is physiological. Delayed defibrillation reduces survival probability in ventricular fibrillation. Excessive interruption of compressions compromises coronary perfusion pressure. Premature medication disrupts the intended progression between electrical cycles. By defining intervention intervals and sequencing order, ACLS training preserves perfusion continuity and limits variability in care delivery across different teams.
The result is not mechanical adherence to a chart but consistent operational discipline. Structured progression allows clinicians to focus cognitive effort on interpretation and quality control rather than on reconstructing the next step.
Cognitive Load and Predictable Error Patterns
During active resuscitation, clinicians must simultaneously interpret rhythm morphology, track medication intervals, monitor compression quality, anticipate defibrillation readiness, and identify reversible causes. Working memory has finite capacity, and when that capacity is exceeded, predictable error patterns emerge.
One pattern involves omission, in which critical reassessment or medication timing is delayed. Another involves sequencing disruption, where interventions occur out of order and compromise physiological optimisation. These failures reflect overload rather than incompetence.
ACLS training reduces this burden by externalising timing intervals and rhythm-based progression. Defined reassessment cycles interrupt fixation on a single interpretation and prompt deliberate evaluation at structured points. In this way, the algorithm functions as a cognitive stabiliser during periods of high environmental intensity.
Rhythm-Specific Control in ACLS Training
A central objective of ACLS training is disciplined management according to arrest rhythm. Each electrical pattern reflects a different underlying physiological failure, and intervention sequencing must align precisely with that pattern. Mastery in advanced cardiovascular life support depends on recognising these distinctions and applying the correct pathway without drift in timing or escalation.
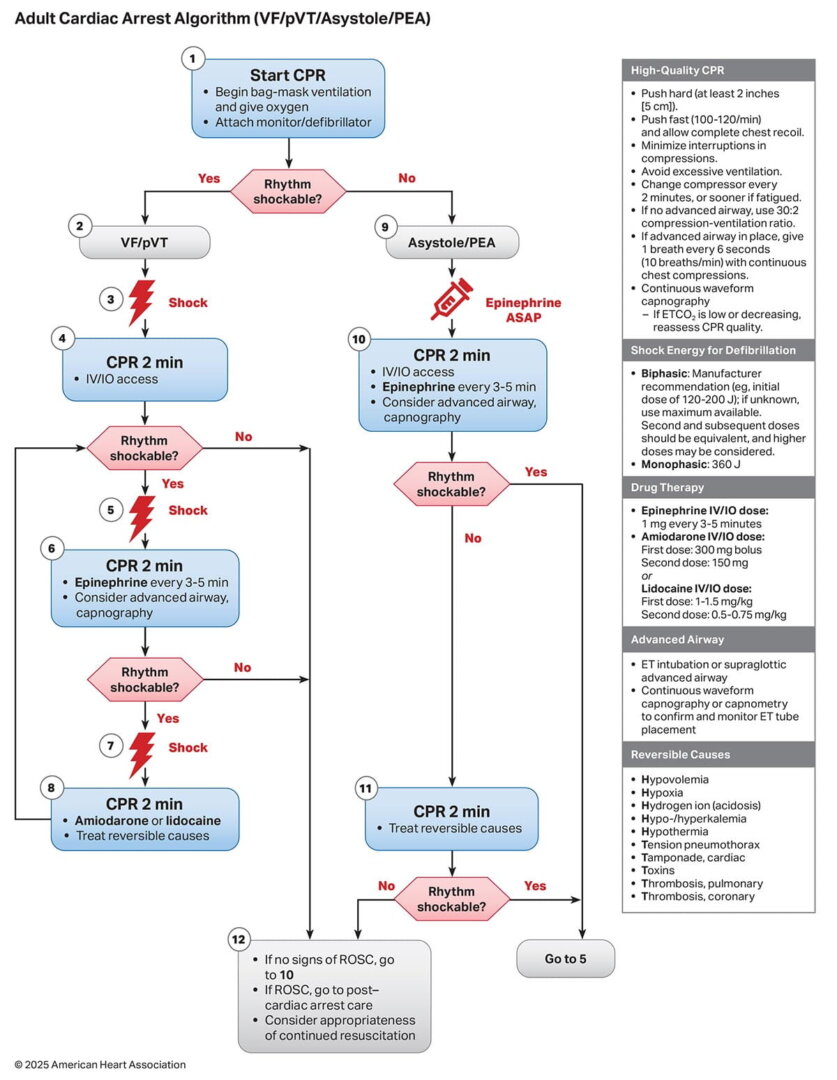
Shockable Arrest – Defibrillation-Driven Management
Ventricular fibrillation and pulseless ventricular tachycardia require rapid electrical correction integrated into a tightly controlled compression cycle. ACLS training reinforces early defibrillation, immediate return to high-quality compressions, and clearly defined intervals before rhythm reassessment.
Medication is introduced within a regulated progression so that pharmacologic support complements electrical therapy. When shock delivery is delayed, pauses extend beyond acceptable limits, or medication disrupts the cycle prematurely, perfusion pressure declines and survival probability falls. Structured sequencing prevents these deviations and preserves compression continuity.
Non-Shockable Arrest – Perfusion and Cause Identification
Pulseless electrical activity and asystole demand a fundamentally different emphasis. Electrical therapy does not correct these rhythms. The priority shifts to circulatory support, timely epinephrine administration, and systematic evaluation for reversible causes.
ACLS training conditions clinicians to maintain strict reassessment intervals while actively investigating factors such as hypoxia, hypovolaemia, metabolic imbalance, tension pneumothorax, massive pulmonary embolism, or toxic exposure. Compression quality and perfusion support remain continuous focal points throughout this evaluation. The structured pathway prevents unnecessary intervention while ensuring that treatable causes are not overlooked.
Peri-Arrest Instability – Escalation Before Collapse
Not all high-acuity events involve pulseless arrest. Severe bradycardia with haemodynamic compromise and unstable tachyarrhythmias can deteriorate rapidly if escalation is delayed.



ACLS training defines:
- Criteria for immediate synchronised cardioversion
- Indications for pharmacologic therapy
- Thresholds for escalation when instability persists
Clear escalation criteria reduce indecision and align intervention intensity with the severity of haemodynamic compromise. Early, structured response in this phase often prevents progression to full cardiac arrest.
Team Leadership and Coordinated Performance in ACLS Training
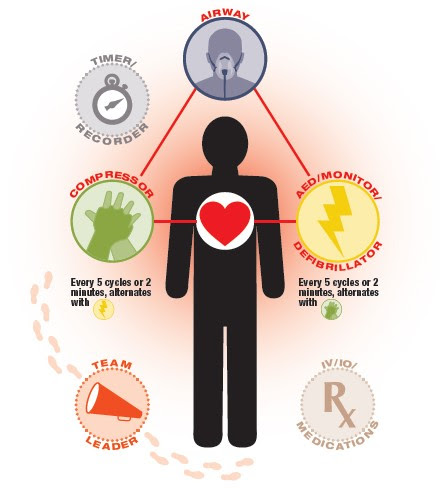
Cardiac arrest management is collective execution under time pressure. High-quality compressions, airway control, rhythm analysis, medication preparation, and documentation occur simultaneously, and each component influences the others. ACLS training recognises that outcomes depend as much on coordinated performance as on individual technical skill.
Shared Mental Model and Role Clarity
A defining feature of effective resuscitation teams is a shared understanding of the current phase of care and the anticipated next step. The ACLS algorithm provides that common reference point. When every team member understands the rhythm category and its corresponding pathway, communication becomes anticipatory rather than reactive.
Junior clinicians are able to prepare medications or defibrillation equipment before direct instruction. Experienced practitioners can allocate attention to compression quality, airway optimisation, and cause identification rather than continuously issuing sequencing commands. This shared structure reduces conflicting directives and preserves momentum during active resuscitation.
Leadership Under Physiological and Environmental Strain
The team leader must maintain oversight of rhythm progression, intervention timing, and evolving haemodynamic response while also monitoring overall team performance. Environmental noise, emotional intensity, and physical fatigue compound this responsibility, particularly during prolonged arrests.
ACLS training supports leadership stability by externalising sequencing decisions. With the algorithm defining the order of interventions and reassessment intervals, the leader’s cognitive resources can be directed toward quality control, identifying reversible causes, and adjusting strategy based on physiological response. This preserves situational awareness when decision density is highest.
Performance Consistency During Extended Arrests
As resuscitation efforts continue, fatigue and stress accumulate. Compression depth may deteriorate, reassessment intervals may lengthen, and communication may fragment. Structured adherence to ACLS protocols sustains rhythm checks, medication timing, and escalation thresholds even as individual stamina declines.
Consistency over time is a measurable outcome of effective ACLS training. It reflects disciplined adherence to defined intervals and progression rather than reliance on memory alone.
Post-Resuscitation Management and Clinical Transition
Return of spontaneous circulation marks a shift in physiology rather than a resolution of risk. Myocardial function is frequently impaired after prolonged arrest, systemic perfusion may remain unstable, and recurrent arrhythmias are common during the early post-arrest period. ACLS training extends beyond pulse restoration by preparing clinicians to stabilise this vulnerable phase with the same procedural discipline applied during active resuscitation.
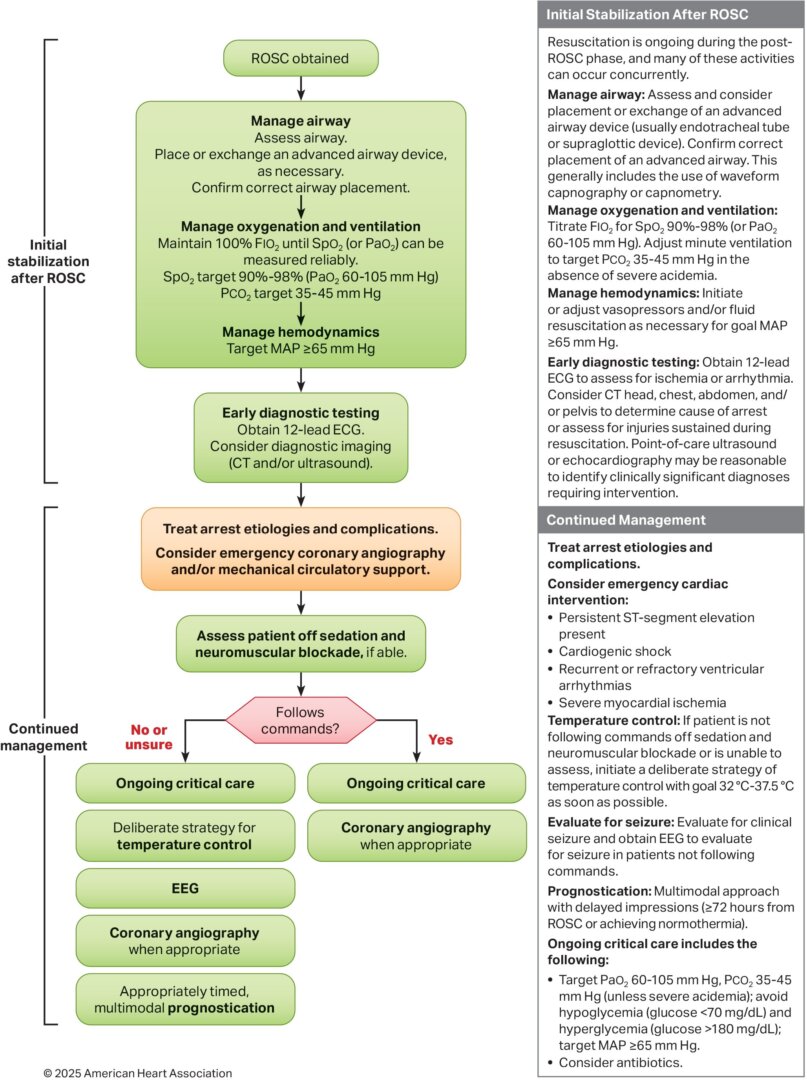
Haemodynamic Stabilisation
Following circulation return, blood pressure often fluctuates due to myocardial stunning, vasodilation, or residual metabolic disturbance. Structured management includes continuous monitoring, titration of vasoactive support when required, and reassessment of perfusion markers such as mental status, urine output, and lactate trends.
Sustained hypotension increases the risk of secondary organ injury. Timely correction requires coordinated monitoring and deliberate adjustment rather than reflex escalation.
Oxygenation and Ventilation Control
Ventilation strategy after resuscitation directly influences cerebral perfusion and neurological outcome. Excessive ventilation reduces venous return and can compromise cerebral blood flow, while inadequate oxygen delivery compounds hypoxic injury.
ACLS training reinforces controlled ventilation rates, avoidance of hyperventilation, and continuous monitoring of oxygen saturation and end-tidal carbon dioxide. Careful titration protects both myocardial recovery and neurological integrity.
Neurological Protection and Cause Identification
Once circulation is stabilised, attention turns to limiting secondary brain injury and identifying the precipitating cause of arrest. Temperature management strategies, glucose regulation, and early diagnostic evaluation form part of this structured transition.
Identifying the underlying driver—whether acute coronary occlusion, pulmonary embolism, metabolic collapse, or toxic exposure—guides definitive management and reduces recurrence risk. The discipline instilled during arrest management carries forward into this diagnostic phase, preserving vigilance when visible urgency decreases.
Clinical Judgement Within Algorithm Boundaries
ACLS algorithms are built on population-level evidence and standardised rhythm categories. Clinical presentation, however, is influenced by patient-specific pathology that may not conform neatly to textbook patterns. Effective ACLS training strengthens judgement within these structured boundaries.
Recognising When Underlying Pathology Alters Priority
Persistent pulseless electrical activity accompanied by rising airway pressures may suggest obstructive pathology. Refractory instability after initial stabilisation may indicate ongoing haemorrhage, toxin exposure, or metabolic disturbance. In such cases, strict mechanical progression through the pathway without deeper evaluation risks missing the true driver of collapse.
ACLS training emphasises active assessment for reversible causes throughout resuscitation rather than treating rhythm in isolation. Clinical reasoning refines the pathway without abandoning its structure.
Informed Adaptation Versus Disorganised Deviation
There is a critical distinction between structured adaptation and uncoordinated departure from protocol. Informed adaptation occurs when a clinician identifies a specific physiological trigger and integrates targeted intervention while maintaining rhythm checks, compression quality, and medication timing.
Disorganised deviation introduces variability without alignment to perfusion status or underlying cause. It fragments team coordination and increases error risk.
Advanced cardiovascular life support training strengthens this discernment. Familiarity with the algorithm establishes a stable operational baseline from which precise adjustments can be made without destabilising the broader resuscitation effort.
HSTCSA – Applying the ACLS Algorithm Through ACLS Training
For healthcare professionals responsible for managing cardiac arrest and high-acuity cardiovascular emergencies, structured ACLS training is essential. The Health and Safety Training Center of South Africa provides American Heart Association–aligned ACLS courses designed to strengthen rhythm recognition, intervention timing, resuscitation leadership, and post-arrest management competence.

Through supervised assessment and evidence-based instruction, participants develop the practical proficiency required to deliver consistent, high-quality advanced life support in demanding clinical environments. Certification confirms measurable competence and alignment with current resuscitation standards.
If your ACLS certification requires renewal, or if you are seeking formal provider qualification, enrolling in an upcoming ACLS training course ensures you remain prepared to manage complex cardiovascular emergencies with confidence and precision.